














Normal Pressure Hydrocephalus
Daniel Walsh FRCS | Consultant Neurosurgeon
Diagnosing Normal Pressure Hydrocephalus and Achieving Better Quality of Life with CSF Diversion Surgery. Content written by Dr Daniel Walsh.
Normal Pressure Hydrocephalus (NPH) is one of the few reversible causes of dementia; however, its name is inherently misleading. While 'hydrocephalus' suggests high pressure, NPH occurs at normal pressure levels. While scans may suggest permanent tissue loss, the clinical reality is often a treatable fluid imbalance.
It was first described as a single case report by a Colombian neurosurgeon, Salomón Hakim in 1957. The condition was defined by a clinical syndrome consisting of three features- unsteady gait, continence problems and dementia. In the years that followed documentation of the condition often reported cases where not all three were present, leading some to doubt the condition really existed and there was frequent difficulty in distinguishing it from other conditions such as Parkinson's disease and other types of dementia.
Signs and Symptoms
This uncertainty persists to the modern day and fundamentally NPH remains a clinical diagnosis as investigations and imaging are of limited help. In our practice we rely on an opinion from an expert neurologist as well to ensure mimics such as Parkinson's disease are reasonably excluded.
Difficulty Walking
Worsening balance when walking is typically the earliest evidence of NPH.
The problem develops gradually and is typically seen in those over 60 years of age although rare cases at a younger age have been reported albeit still over the age of 40 years.

The characteristic gait is sometimes described as "magnetic"- as though the feet were stuck to the ground and difficult to lift up. The stance becomes broad-based and turning 180 degress becomes difficult requiring three or more adjustments. Alternative causes such as spinal pathology should be excluded by a combination of physical exam and imaging.
Cognitive Impairment
There may be behavioural changes or difficulty in performing multistep procedures, working memory, formulation of abstractions/similarities as well as insight into these problems.
Recall of recent events may become increasingly difficult. There may also be difficulty with fine motor movement including in the hands and a generalised slowing in tasks which is easy to confuse with the bradykinesia seen in Parkinson's disease.
All of these changes can be documented using standardised questionnaires and again other conditions capable of mimicking these problems need to be excluded in so far as possible.
Incontinence
Urinary or fecal incontinence can occur intermittently or persist. It is crucial to investigate other potential causes, such as weak pelvic muscles or prostate issues. Consulting a urologist is essential for an accurate diagnosis.
Investigations
Assessment by an expert neurologist is an essential element of any evaluation. If the clinical picture fits then the following investigations will help close in on the diagnosis and determine if shunt surgery is likely to be helpful.
CT scan
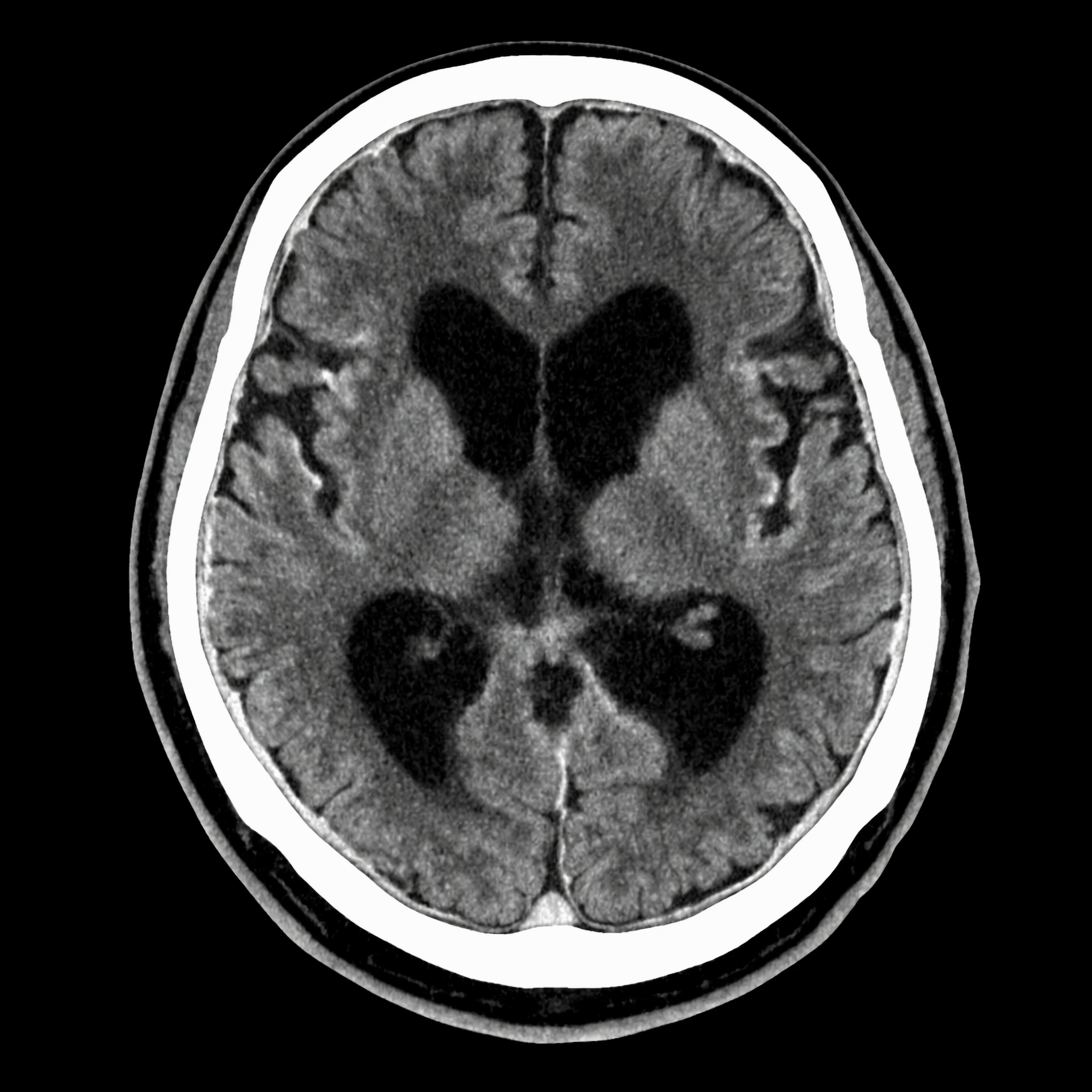
CT scans can be done in a short time, something that may be useful if the subject is uncomfortable lying still or is claustrophobic. The ventricles and other spaces containing cerebrospinal fluid are well demonstrated although the detail of cerebrospinal fluid flow and of the geography on the surface of the brain is not as detailed as with MRI.
CT could be the investigation of choice if assessing shunt function in an emergency or if there is a concern about bleeding following surgery.
MR Imaging
MRI does not use x-rays but rather exploits differences in the water content of tissues to create detailed images. It requires the subject to sit within a strong magnetic field for a period of time and depending on the information being sought the scan can take rather longer than a CT scan.
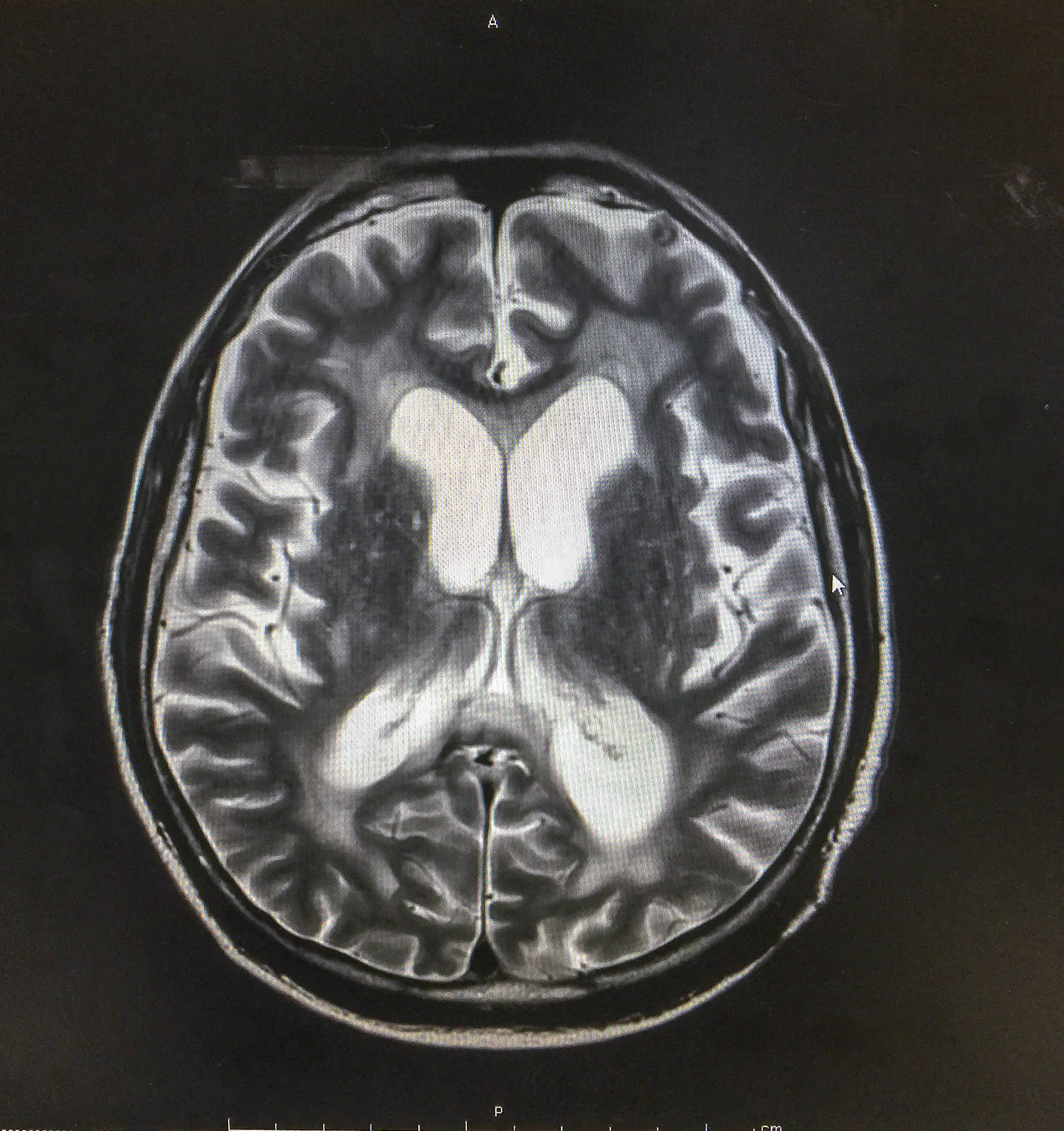
While scan images alone cannot confirm the diagnosis of NPH there are appearences on MR suggestive of the condition which must be interpreted in context with the clinical exam and other tests below. There are a range of conditions that may produce similar appearences on an MRI and which may also need to be ruled out before CSF diversion surgery can be recommended.
CSF Investigations
The response to reducing the amount of cerebrospinal fluid (CSF) is central to securing the diagnosis of NPH. it is not entirely understood how the handling of CSF by the nervous system brings about these symptoms and it is not simply the case that pressure increases within the brain owing to an overproduction of CSF. The pressure when measured at a single time-point is typically not elevated above that normally encountered in helathy individuals.
Lumbar Puncture ("Tap" Test)
A lumbar puncture is typically performed under local anesthesia. Approximately 40ml of CSF is removed, and the measured pressure is usually not significantly elevated. Occasionally, x-ray guidance is needed, especially if there has been previous spinal surgery or significant spinal column disease.
It is routine to send a fluid sample for basic chemical tests and to rule out infection, although it is unlikely anything will be found amiss. After the lumbar puncture, you will be asked to lie flat for about two hours. Over the next 24 hours, it is advisable to drink plenty of clear fluids to prevent a headache from developing due to low pressure inside the head. If a headache develops that improves when lying flat, it will usually resolve spontaneously, but if it persists beyond 24 hours, inform your doctor as additional remedies may occasionally be needed.
Before the lumbar puncture, physiotherapy and occupational therapy are typically conducted to establish parameters for measuring the response. These may include cognitive screening tests, but the most sensitive is a timed walking assessment. These tests will be repeated after recovery from the lumbar puncture to determine if there is an improvement in walking speed and gait pattern. Sometimes, performance in cognitive tests improves, or family members may notice differences for a few days after the test.
Continuous CSF drainage
In cases where the results of a tap test are inconclusive, extended continuous CSF drainage may identify candidates who could still benefit from CSF diversion surgery.
The procedure to place a lumbar drain is very similar to a lumbar puncture except that a small silicone catheter is left in placed in the spinal canal and tunnelled out under the skin where it is connected to a collection bag. The amount drained is regulated by a pump or by intermittently opening the tap on the system and allows for near continuous drainage over a period of days, mimicking the effect of placing a shunt internally.
The drawback of this procedure is a small risk of introducing infection into the CSF or of overdraining the fluid.
CSF Infusion Studies
This requires placement of a catheter as described above. This catheter is then connected to pump that allows for the infusion of sterile fluid over a period of time while a pressure sensor connected to the system measures the resistance to that flow. The resulting pressure curve can indicate that an individual with the clincial features of NPH might benefit from a shunt and it may be more sensitive than the tap test alone. As it does carry a small amount of additional discomfort and risk it is usually reserved for when the results of a tap test are equivocal. Read about the NICE guidance pertaining to lumbar CSF infusion studies here.
Surgical Treatment
The definitive treatment of NPH is a procedure usually termed a "shunt". The goal of this surgery is to divert CSF from the brain or spinal canal into another anatomical space where it can be re-absorbed by the body.
What is a Ventriculo-peritoneal Shunt?
A catheter is placed into the ventricles, chambers in the brain where CSF is manufactured, and then connected it to a valve to regulate the amount of fluid draining and implant another catheter in series into the abdomen where the lining of the body cavity is capable of efficently absorbing the CSF.
If the abdominal cavity is not available e.g. by reason of scarring after infection or extensive surgery, then the chest cavity may be used or fluid plumbed directly into a vein. If the ventricles are too small to safely navigate, a catheter can be placed in the lumbar spinal canal and tunnelled into the abdomen.
Will a Shunt Help My NPH?
The PENS Trial- A randomised controlled trial compared a group with NPH who received a VP shunt to a group who recieved a shunt with the valve temporarily closed. At 3 months shunting resulted in significant improvements in gait velocity and a measure of gait and balance but not in measures of cognition or incontinence. It was also effective in reducing falls by about half.
There are less rigrorous studies suggesting benefits to cognitive performance but this trial allows us to offer shunt surgery with a good degree of confidence that patients will benefit in terms of their mobility. This may not last for ever but the use of progammable valves that can be adjusted to increase flow over time may prolong the effect. They also assist in managing some of the complications of shunt surgery.
What are the Risks of a VP Shunt for NPH?
Although generally very safe a shunt is still a neurosurgical procedure and carries some risk.
- Risk to life- at around the time of surgery is reported at 1-3% and is very dependent on the medical fitness of the subject taking account that many people undergoing this surgery are of advanced age.
- Neurological Worsening- can occur due to bleeding in the brain during catheter placement or misplacement. The estimated risk is about 5%.
- Seizures- can result from irritation on the surface of the brain. If they occur they will usually be controlled by medication that will then need to continue indefinitely.
- Subdural Blood- gradually collecting on the surface of the brain as the pressure inside reduces due to the shunt. This occurs in 10-12% of cases and may be managed conservatively, with shunt valve adjustment or occasionally it requires surgical removal.
- Infections- Superficial infection involving the skin occurs in about 1% of cases. Infection attaching to the shunt or in the CSF will usually require removal of the shunt, affecting about 5% of procedures.
- Mechanical Failure- shunts may obstruct and require maintence by replacement of components occasionally.


